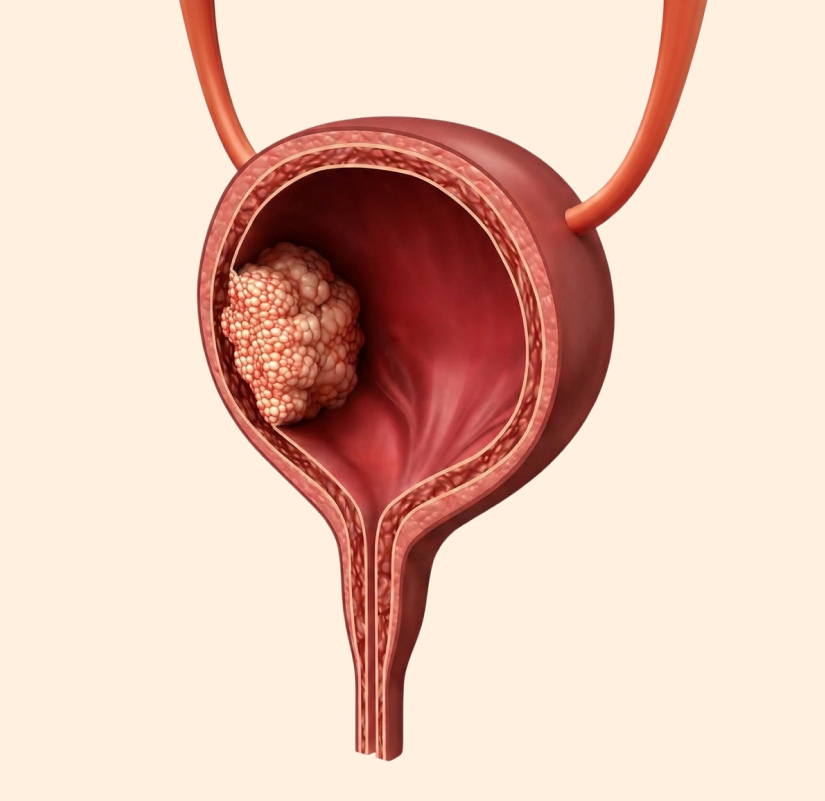
When the disease has grown into the muscular wall of the bladder, organ-preserving strategies may no longer be sufficient to control the cancer effectively.
The standard of care at this stage often involves radical cystectomy, the surgical removal of the bladder. In men, radical cystectomy typically includes the removal of the prostate gland and seminal vesicles as part of the standard procedure. In women, the uterus, ovaries, and part of the vaginal wall may also be removed depending on the extent of disease. After bladder removal, your surgeon will create an alternative pathway for urine to leave your body, called urinary diversion.
Cisplatin-based chemotherapy is strongly recommended before surgery (neoadjuvant chemotherapy) to target microscopic spread and improve survival outcomes. For those who did not receive neoadjuvant therapy and have high-risk pathological features, adjuvant chemotherapy or immunotherapy may be offered after surgery.
In select cases, a bladder-preserving approach combining chemotherapy and radiation therapy may be considered. This is not suitable for every patient, and the decision involves a detailed discussion about potential risks, likelihood of success, and functional outcomes. Drawing on his specialisation in kidney, bladder, and prostate conditions, Dr Azhari guides patients through these complex treatment choices with a focus on balancing disease control with long-term quality of life.